What to Consider Before Getting a COVID-19 "Vaccine" or Semi-Annual Re-Vaxx
There will be likely a need for a third [COVID-19 "vaccine"] dose, somewhere between 6 and 12 months. And then from there. There will be an annual revaccination. But all of that needs to be confirmed.
In prior pieces, I've referred to the products du jour here as COVID not-vaccines [*3], as I do not believe these products qualify to be ascribed the commonly-understood definition of "vaccine" the public is familiar with. For simplicity sake, in this piece, I'll be using the newly-updated definition of "vaccine," which more squarely allows the COVID-19 immunity-stimulation products we call "vaccines" to qualify for the label. Apples and pears are both fruit. If the dictionaries redefine pear to also mean apple, I suppose we can consider pears as apples. Thus, I'll drop my quotation marks around the label vaccine going forward. But my readers should be aware of the conflicting definitions and gradual re-definition, broadening the term over the early twenty-first century.
A caveat. If I were discussing general public law that might relate to an individual I haven't spoken with, I'd disclaim that my general legal opinion on issues affecting millions of Americans should not be construed as one-on-one legal advice, even though I'm licensed to give it. Since everyone's legal situation is unique, there is no one-size-fits-all solution legally, as everyone has countless permutations that could factor into my advice if applied to an individual as opposed to speaking on a general level.
I imagine the same applies to medicine. Each human body is unique, and medicine for it can have different effects for different people, which would include vaccines. Thus, even if I were an expert physician on vaccines, which I am not, I'd still qualify my opinion by suggesting readers check with their doctors on the matter for vaccine information specific for their unique human body. But, their doctors, like their lawyers on legal matters, could always be wrong. Thus, medical, just like legal decisions, are always personal matters. If this wasn't so, there would be no need for "second opinions," and we wouldn't call it a medical "opinion" in the first place, but a fact.
NOTE: as of August 14, 2021, this piece is completed and has four parts you may click and read independently:
Part 1: If the COVID-19 Vaccines Are Dangerous, How Come the Media Isn't Telling Us?
Part 2: False Efficacy: the Difference Between Absolute and Relative Risk
Part 3: Adverse Effects: the Seen and the Unseen
Part 4: Immunity for Them, Not for You
Or, you may read all four parts by continuing below...
#1 If the COVID-19 Vaccines Are Dangerous, How Come the Media Isn't Telling Us?
As of May 21, 2021, despite being a fraction of the billions upon billions of vaccines given since 1990 in the United States, COVID-19 vaccines represented 46.06% of all death (4,265 out of 9,258) and 21.65% (3,284 out of 15,165) of all permanent disability incidents reported since 1990 to the Centers for Disease Control and Prevention's (CDC) Vaccine Adverse Event Reporting System (VAERS) [*4], a voluntary-reporting tool healthcare workers and individuals may use if they believe a vaccine may have caused an injury or death (meaning not all possible incidents are recorded). COVID-19-vaccine incidents in the U.S. total 248,947, or 24.8% of all incidents reported since 1990, as of publication of this piece (UPDATE: as of, July 30, 2021, they total 40.9% worldwide on VAERS, with 603,686 incidents). This percentage rapidly increases as we progress further into 2021 and beyond. You won't read about this most places, but the data can be readily accessed here [*5].
A report to VAERS doesn't necessarily mean the injury or death after a COVID-19 vaccine was definitively caused by that vaccine. But how many incidents are not reported to VAERS? A 2010 report on the VAERS system, submitted to a federal agency, stated [*6]:
Why don't the vast majority of the media report negative COVID-19 vaccine information? It's important to recognize that you are not the customer. You are the product being delivered to the real customer: advertisers that include pharmaceutical companies with a vested financial interest in being paid for as many vaccine doses as possible.[F]ewer than 1% of vaccine adverse events are reported. … Barriers to reporting include a lack of clinician awareness, uncertainty about when and what to report, as well as the burden of reporting: reporting is not part of the clinician's usual workflow, takes time, and is duplicative.
Robert F. Kennedy, Jr., lawyer and vaccine-safety advocate, describes the dilemma in shocking detail in his foreword to Dr. Joseph Mercola's May 2021-published book, The Truth About COVID-19 [*7]:
Big Pharma’s $9.6 billion annual advertising budget gives these unscrupulous companies control over our news and television outlets. Strong economic drivers (pharmaceutical companies are the biggest network advertisers) have long discouraged mainstream media outlets from criticizing vaccine manufacturers. In 2014, a network president, Roger Ailes, told me he would fire any of his news show hosts who allowed me to talk about vaccine safety on air. "Our news division," he explained, "gets up to 70% of ad revenues from pharma in non-election years [emphasis added]."Regarding social media companies' constant censorship and "fact checking" to ensure their readers (i.e. their human products they sell to advertisers) won't doubt the safety and/or efficacy of COVID-19 vaccines, these companies are funded by advertisers that use the platforms to target specific people, including people that researched information on particular drugs. The Washington Post reported on March 4, 2020 [*8], "Spending on Facebook mobile ads alone by pharmaceutical and health-care brands reached nearly a billion dollars in 2019, nearly tripling over two years, according to Pathmatics, an advertising analytics company [emphasis added]." Advertisers go as far as to bully social media companies for not actively censoring "misinformation" about their products. According to Pfizer, one the biggest COVID-19 vaccine makers, as CBS reported on June 30, 2020 [*9]:
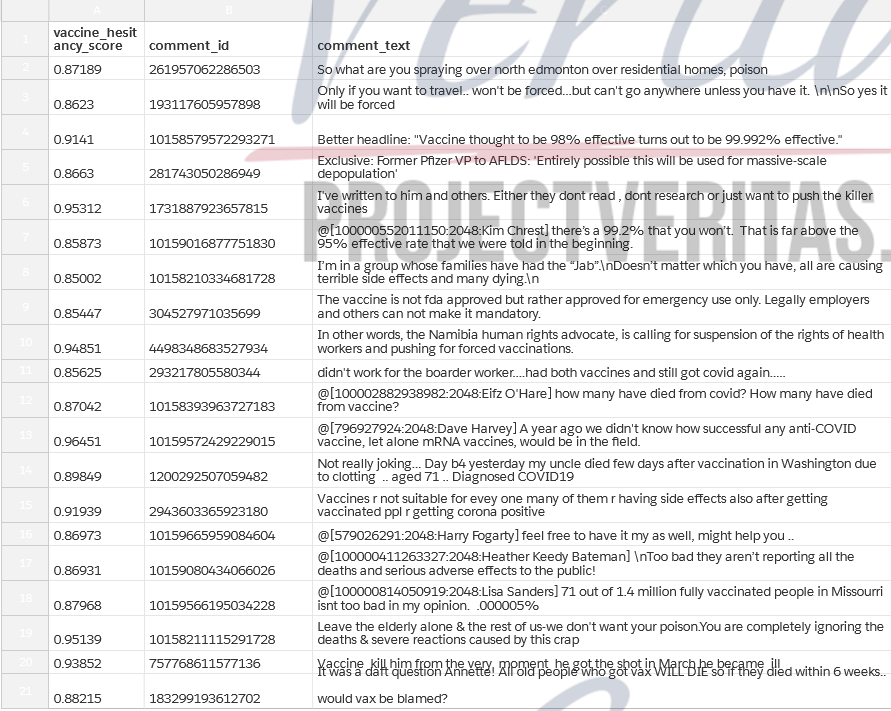
Pfizer said it will be removing all of its advertising from Facebook and Instagram for the month of July. “Today, we are asking Facebook to take proactive steps to ensure their platforms are safe and trusted spaces for all,” the company said.And, Facebook and Instagram at least, not only bent the knee to Big Pharma but lowered both knees and assumed the position for them. In leaked documents from Facebook, released by Project Veritas on May 24, 2021 [*10], we learned Facebook actively removes or demotes comments by users sharing information they refer to as "vaccine hesitancy" via a trial program affecting 1.5% of their 3.8 billion world-wide users. The document reveals 19.42% of comments on pages discussing vaccination are negative or "vaccine hesitancy." Such comments represent 25.3% of those on "Health Authority Pages." Despite these comments being the minority, Facebook states a goal of reducing them further.

Comments that are anti-vaccine are outright removed, depending on their user-reach and level of discouragement, while comments that are true but not actively discouraging taking the vaccine, like personal stories about negative effects or factual information that's negative to the vaccines, are "demoted." This means hidden from other viewers, or, as it's colloquially referred to, "shadow banned."


Pages, groups, or accounts explicitly dedicated to discouraging vaccination are "removed" if they become too visible, while non-explicit vaccine-discouraging accounts simply have their comments related to "vaccine hesitancy" made less visible to the general public.
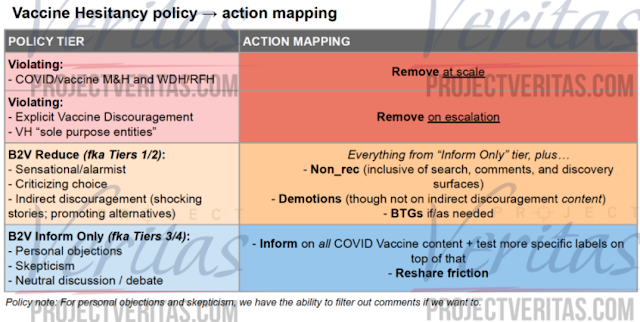
There's even a scoring system applied to comments for deciding what action the censorship algorithms will take.
We're all familiar with the labels social media puts on posts users share on any topic even tangentially related to COVID-19 vaccines, reminding us of how safe and effective they are alleged to be. We're also familiar with the "fact checks" they add to any negative vaccine information, to reassure us there is either another side of the argument or the article shared is "false," "mostly false," or (my favorite) "missing context."
The social-media pleas they self-refer to as "fact checks" on COVID-19 vaccines are to ensure their customers (pharmaceutical companies) advertise on their platforms. But they are laughably inept. Even the "fact checks" from the general more-reputable media are feckless. Take this Reuters "fact check" on whether the vaccines prevent human-to-human-transmission of COVID-19 [*11]. Reuters admits the vaccines were never tested on human-to-human transmission (which, one would think, disqualify said pharmaceutical products from the label "vaccine") [*12] but argues that, because there is no evidence the labeled vaccines don't prevent human-to-human transmission, claims saying they don't are false.
There is no proof snake oil triples the size of the male penis, but, because there is no proof snake oil doesn't do this, doubting the veracity of the claim is false! See how this works? The aforementioned Reuters "fact check" is so feckless and wickedly dishonest, I screenshot it below, as it dispels belief when merely quoted.


The heuristic regarding the efficacy of substituting the word of authorities for foundational knowledge is usually a sound shortcut to navigate life decisions, since we can't critically examine everything we claim to "know" [*13]. We rely on news reports, papers, and books we commonly refer to as "authorities" to inform us as a proxy. We don't have the time or knowledge-base, let alone legal authority, to create pharmaceutical products in our basements, run experiments at home, and find 100,000 test subjects to track efficacy and safety of our creations. So, we trust the conclusions of authorities that have done similar things for us, who could easily get their data, let alone their conclusions from that data, wrong. How wrong? The UC San Diego News Letter reports [*14]:
[A May 21, 2021-published study *15] analyzed data from three influential replication projects which tried to systematically replicate the findings in top psychology, economic and general science journals (Nature and Science). In psychology, only 39 percent of the 100 experiments successfully replicated. In economics, 61 percent of the 18 studies replicated as did 62 percent of the 21 studies published in Nature/Science.If the raw data the conclusions we call "science" are that inaccurate, imagine how much worse the sophistry of pharmaceutical-funded media and social media companies who relay this kind of information is?
#2 False Efficacy: the Difference Between Absolute and Relative Risk
As mentioned in part #1, most should be aware that COVID-19 (COVID) vaccines were never tested on human-to-human transmission. The chief medical officer at Moderna, Tal Zaks, excuses this neglect on testing [*1]: “Our trial will not demonstrate prevention of transmission, because in order to do that you have to swab people twice a week for very long periods, and that becomes operationally untenable.” It's now too late to find out whether or not transmission occurs after vaccination, as the original placebo group could get the "real" vaccine after the clinical trials for "emergency use" ended.
The FDA first approved the Pfizer COVID vaccine for emergency use on December 11, 2020 [*2]. But, Pfizer compromised its control group in its trials a month earlier. Nature reports [*3]:
This not only invalidates future assessments on human-to-human transmission but also those regarding long-term health effects. Lack of data on transmission and long-term effects is why COVID vaccines are approved by the Food and Drug Administration (FDA) for "emergency use" only, and the makers are immune from liability (more on that in a part to follow).On 10 November [2020], Pfizer sent a letter to participants, seen by Nature, which states that the company is exploring ways to allow interested participants in the placebo group who meet eligibility criteria for emergency access to cross over into the trial’s vaccine arm. A spokesperson told Nature that the company would have “an ethical responsibility to inform all study participants about the availability of an Emergency Authorized Vaccine.”
Nonetheless, you've probably read that COVID vaccines are about 95% effective. What does that mean?
In order to measure vaccine effectiveness, we must first determine what the vaccines are "effective" upon. COVID cases are diagnosed using a polymerase chain reaction (PCR) test. A swab of ribonucleic acid (RNA) is collected from deep inside the nose and reverse-transcribed into deoxyribonucleic acid (DNA), which is then used to detect traces of the COVID virus. To be discernible, the sample needs to be amplified in rounds. The number of amplifications is called the cycle threshold (CT). The higher the number, the more sensitive the test is and the more likely it results in a false positive. In Dr. Joseph Mercola's book, The Truth About COVID-19, at pages 78-79 [*4], his co-author, Ronnie Cummins elaborates:
A September 28, 2020, study in Clinical Infectious Diseases revealed that when you run a PCR test at a CT of 35 or higher, the accuracy drops to 3 percent, resulting in a 97 percent false positive rate. Yet tests recommended by the World Health Organization are set to 45 cycles, and the US Food and Drug Administration and the US Centers for Disease Control and Prevention recommend running PCR tests at a CT of 40. The question is why, considering the consensus is that CTs over 35 render the test useless. …
[A]n April 2020 study in the European Journal of Clinical Microbiology and Infectious Diseases showed that to get 100 percent confirmed real positives, the PCR test must be run at 17 cycles. Above 17 cycles, accuracy drops dramatically. By the time you get to 33 cycles, the accuracy rate is a mere 20 percent, meaning 80 percent are false positives. Beyond 34 cycles, your chance of a positive PCR test being a true positive shrinks to zero. According to a December 3, 2020, systematic review published in the journal Clinical Infectious Diseases, no live viruses could be found in cases where a positive PCR test had used a CT above 24.
Here is the graph from the paper referenced, suggesting a CT of 17 is preferable [*5].

Cummins summarizes the problems with PCR testing on page 77 [*6]:
At present, the polymerase chain reaction test is the primary method used to test people for COVID-19. The problem with that is twofold. First of all, the PCR test cannot distinguish between inactive viruses and “live” or reproductive ones. This is a crucial point, since inactive and reproductive viruses are not interchangeable in terms of infectivity. If you have a nonreproductive virus in your body, you will not get sick and you cannot spread it to others. For this reason, the PCR test is grossly unreliable as a diagnostic tool.
As I've written before [*7], over the summer of 2020, Florida COVID cases went from 2,000 to 12,000 per day, at the same time multiple testing sites featured a positivity rate of close to 100%, including Orlando Health, which reported 98% positive tests and had to correct its records down to 9.4% [*8]. In a study published by the International Journal of Geriatrics and Rehabilitation, the CDC's COVID test kits were found to give inaccurate results 50% of the time, a 30% false positive rate and 20% false negative [*9].Second, many if not most laboratories amplify the RNA collected far too many times, which results in healthy people testing positive. In order for the PCR test to be of any use whatsoever, in terms of diagnosing COVID-19, labs would need to considerably reduce the number of amplification cycles used.
On January 20, 2021, the day before Joe Biden's inauguration, the World Health Organization (WHO) updated its guidance on PCR tests for COVID to be more cautious of false positives and to ensure "clinical observations" (i.e. symptoms) are considered as well before making a diagnosis [*10]:
Still, positive COVID tests have negative ramifications for their victims, regardless of any symptoms detected and regardless of having previously received COVID vaccinations.WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT [nucleic acid testing] technology.WHO reminds IVD [in vitro diagnostic medical device] users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers must consider any result in combination with timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information [emphasis added].

Without symptoms, we call a person with a positive PCR test "asymptomatic" and assume he can spread the virus anyway, a supposition with not only no clinical evidence to back it but evidence disproving it [*11]:
So, how was a COVID case determined in the clinical trials for the vaccines? Because adverse reactions are common in the COVID vaccines, how can we know if a trial subject who exhibited flu-like symptoms, such as myalgia, fever, headache, and chills is suffering from an adverse reaction to the vaccine as opposed to COVID itself or some other illness? Peter Doshi at BMJ, a resource for healthcare professionals, found alarming language in Moderna's trial instructions [*12]. Moderna explains on page 62 [*13]:In this study, we recorded in detail the hospitalized situation, diagnostic procedure, inspection results, treatment plans and clinical outcome of an asymptomatic SARS-CoV-2 carrier who was laboratory confirmation by RT-PCR assay, but without related symptoms and imaging changes in concert with previous reports. Also, we analyzed epidemiological and clinical data from 455 contacts who had been exposed to the asymptomatic patient. All the 455 contacts were excluded from SARS-CoV-2 infection. Of the 231 quarantined people (196 family members and 35 patients), 229 were removed from medical observation successfully and two died for severe heart failure. New or existing respiratory symptoms were almost appeared in patients, which were considered to be associated with their original disease or complications. A family member complaining of fever was diagnosed as acute tonsillitis ultimately. Unlike COVID-19, normal blood count was found in most contacts. All CT images showed no sign of COVID-19 infection. Unquestionably, all cases tested negative for SARS-CoV-2 nucleic acid. This fact illustrated that there had been no cases of infection in a relatively dense space [emphasis added].
Not all symptomatic subjects in the vaccinated groups were PCR tested. And, for those that were tested, what were the CTs for those PCR tests in any the clinical trials? They were not disclosed [*14].It is important to note that some of the symptoms of COVID-19 overlap with solicited systemic ARs [adverse reactions] that are expected after vaccination with mRNA-1273 (eg, myalgia, headache, fever, and chills). During the first 7 days after vaccination, when these solicited ARs are common, Investigators should use their clinical judgement to decide if an NP [nasopharyngeal] swab should be collected. The collection of an NP swab prior to the Day 1 and Day 29 vaccination can help ensure that cases of COVID-19 are not overlooked. Any study participant reporting respiratory symptoms during the 7-day period after vaccination should be evaluated for COVID-19.
Now that we have a vague idea of what the vaccines must be "effective" against, we must further distinguish between absolute and relative risk of COVID. Absolute risk is the probability one will get COVID when measured against the general population. Relative risk is the difference in getting COVID measured between those getting a COVID vaccine and those getting a saline injection (placebo, control group). When the vaccine makers refer to 95% efficacy, they are referring to relative risk.
Dr. Gilbert Berdine, MD, associate professor of medicine at Texas Tech University Health Sciences Center elaborates [*15]:
The Pfizer study had 43,538 participants and was analyzed after 164 cases. So, roughly 150 out [of] 21,750 participants (less than 0.7 percent) became PCR positive in the control group and about one-tenth that number in the vaccine group became PCR positive. The Moderna trial had 30,000 participants. There were 95 “cases” in the 15,000 control participants (about 0.6 percent) and 5 “cases” in the 15,000 vaccine participants (about one-twentieth of 0.6 percent). The “efficacy” figures quoted in these announcements are odds ratios.
Of course, Pfizer couldn't be overtaken by Moderna, as shortly thereafter, Pfizer released updated results, analyzed by Peter Doshi, showing Pfizer's "efficacy" now matched Moderna's [*16]: "Pfizer says it recorded 170 covid-19 cases (in 44,000 volunteers), with a remarkable split: 162 in the placebo group versus 8 in the vaccine group." What do you know? Both are equally effective at about 95%.
The difference between 162 in the placebo control group and eight in the real vaccinated group in the Pfizer trials equates to 95% effectiveness (8/162 - 1).The difference between 95 in placebos versus five vaccinated in Moderna also equals 95% effectiveness (5/95 - 1). This is what we call relative risk.
How accurate is this relative risk? Recall, symptomatic subjects in the vaccinated group could be excused from PCR testing based on a doctor's assumption that flu-like symptoms were an adverse vaccine reaction instead of a possible case of COVID. Thus, these instances were excluded from the COVID tally, but all came from vaccine group instead of the control group. Hence, there may have been more COVID cases in the vaccine group than actually reported, which would dramatically lower the relative effectiveness.
A more-useful measure would be against absolute risk, meaning the odds the general public will get COVID, vaccinated versus not, or the number of vaccines needed to prevent a single case. If it takes 167 vaccinations to prevent a single "case" of COVID, one person is saved from the symptoms of the disease while 166 are subject to the risks of the vaccine. Even if the risk of harm from COVID itself is greater than the risk of harm from the vaccine (as we assume), the damage from the vaccine to the general population can still be far greater, when we account for a 167:1 ratio.
Dr. Berdine explains [*17]:
When measuring the odds of getting COVID, whether after being vaccinated or not, it's important to also consider the risk of death from COVID [*18].There is no evidence, yet, that the vaccine prevented any hospitalizations or any deaths. The Moderna announcement claimed that eleven cases in the control group were “severe” disease, but “severe” was not defined. If there were any hospitalizations or deaths in either group, the public has not been told. When the risks of an event are small, odds ratios can be misleading about absolute risk. A more meaningful measure of efficacy would be the number to vaccinate to prevent one hospitalization or one death. Those numbers are not available. An estimate of the number to treat from the Moderna trial to prevent a single “case” would be fifteen thousand vaccinations to prevent ninety “cases” or 167 vaccinations per “case” prevented which does not sound nearly as good as 94.5 percent effective. The publicists working for pharmaceutical companies are very smart people. If there were a reduction in mortality from these vaccines, that information would be in the first paragraph of the announcement [emphasis added].

Using the "current best estimate" scenario (as of June 8, 2021), even the CDC concedes the 18-49 age demographic has a 99.95% survival rate, while the 50-64 demographic is at 99.4% and the 65+ demographic has a 90% survival rate. This is, of course, if one contracts COVID. And, as discussed prior, since post-vaccination human-to-human transmission wasn't tested and we know vaccinated people are testing positive for COVID anyway, you are taking the vaccine not to protect others but to reduce your personal risk.
But what about your risk of suffering symptoms from COVID? If the vaccines don't prevent transmission, let alone one contracting the virus, it should at least give recipients a milder case of COVID. Right?
The most common rebuttal you'll get from an educated person who gets a COVID vaccine and recognizes that the product is not designed to prevent his asymptomatic transmission of the virus to others: The virus poses a risk of a severe case to me, involving hospitalization or death, and, because I want to mitigate the risk, I'm taking the vaccine to see that, if I get COVID, I'm more likely to get a more-mild case.
Let's assume that and the "asymptomatic carrier" supposition are true. If someone has more-severe symptoms, they are less likely to be "asymptomatic," meaning they are less likely to leave home and spread the virus to others. With less symptoms, a person might not know he has the virus and be unknowingly spreading the virus to others. Thus, he decreases his probability of hospitalization or death to him while increasing that probability to others.
To make matters worse, many businesses are claiming people that are vaccinated don't have to wear face masks. Assuming face masks reduce alleged "asymptomatic transmission," (which I don't believe is true [*19]), the risk to the unvaccinated population is compounded. Thus, to be effective as a tool of public policy, the whole population of a jurisdiction or the global population would need to be vaccinated. Otherwise, a benefit is conferred to the vaccinated at direct cost to the unvaccinated that face an increased risk of injury or death.
But do the COVID vaccines actually reduce severe symptoms? How could the vaccine trials tell us?
Peter Doshi at the BMJ, [*20], highlights a dilemma:
So, when we only have a few hundred cases of COVID in the trials to measure against hospitalizations occurring in around 4% of cases, we'd probably only see eight hospitalizations. To find out how many we'd be keeping out of the hospital, via measuring the vaccinated versus a placebo control group, we'd only have a handful of possible hospitalizations to analyze. How did the trials handle this dilemma?Severe illness requiring hospital admission, which happens in only a small fraction of symptomatic covid-19 cases, would be unlikely to occur in significant numbers in trials. Data published by the US Centers for Disease Control and Prevention in late April reported a symptomatic case hospitalisation ratio of 3.4% overall, varying from 1.7% in 0-49 year olds and 4.5% in 50-64 year olds to 7.4% in those 65 and over.13 Because most people with symptomatic covid-19 experience only mild symptoms,14 even trials involving 30 000 or more patients would turn up relatively few cases of severe disease.
Doshi elaborates [*21]:
Doshi quotes Moderna's chief medical officer, Tal Zaks [*22], who excuses this practice:In the trials, final efficacy analyses are planned after just 150 to 160 “events,”—that is, a positive indication of symptomatic covid-19, regardless of severity of the illness. ...In all the ongoing phase III trials for which details have been released, laboratory confirmed infections even with only mild symptoms qualify as meeting the primary endpoint definition. 9 10 11 12 In Pfizer and Moderna’s trials, for example, people with only a cough and positive laboratory test would bring those trials one event closer to their completion. (If AstraZeneca’s ongoing UK trial is designed similarly to its “paused” US trial for which the company has released details, a cough and fever with positive PCR test would suffice.)
Doshi concludes:The trial is precluded from judging [hospital admissions], based on what is a reasonable size and duration to serve the public good here. ... Would I like to know that this prevents mortality? Sure, because I believe it does. I just don’t think it’s feasible within the timeframe [of the trial]—too many would die waiting for the results before we ever knew that.
Hospital admissions and deaths from covid-19 are simply too uncommon in the population being studied for an effective vaccine to demonstrate statistically significant differences in a trial of 30 000 people. The same is true of its ability to save lives or prevent transmission: the trials are not designed to find out.
#3 Adverse Effects: the Seen and the Unseen
If the COVID-19 vaccines are less effective than the media proclaims or ineffective (setting aside evidence, as Dr. Robert Malone suggests, that they may be counter-effective via antibody-dependent enhancement [*1]), what's the harm in taking them anyway? Anecdotally, you likely know many people who've taken them and experienced mild side-effects for a day or two that resolved, and some who may have experienced no side effects. If it's free to take one of these emergency-use-authorized vaccines, what have you got to lose by trying one out? How can we measure the societal risk-to-reward ratio in mass COVID-19 vaccination?
Everyone, even those we'd label "pro-vaccine," agrees adverse effects from the COVID-19 vaccines exist. The only questions are: (1) how often, (2) how severe, and (3) for how long? How do we measure these variables? Do severe and/or long-lasting effects kick in only within a few days after receiving a vaccine? Or, can they be seen one month, or, perhaps, years into the future? Years in the future, how would we know if a person is experiencing a health condition (e.g., an enlarged heart muscle, as the U.S. Centers for Disease Control and Prevention (CDC) confesses [*2]) that is causally connected to the vaccine he took years ago? When people say adverse effects are "uncommon," how pervasive must future-reported side effects be before that label would be retracted?
Every day, we learn something new about adverse effects from the COVID-19 vaccines. But, at some point, it's time to pause spectating and start congregating and analyzing information. As of July 30, 2021, here are some critical things we know.
There are two kinds of COVID-19 vaccines being offered. One is the Johnson and Johnson (in the U.S.) and Astrozeneca (in Europe) kind, commonly described as "viral vector" vaccines. Since the world's various organizations tend to take the CDC's word as gospel on the COVID situation, let's see what the CDC proclaims about the viral-vector vaccines [*3].
Notice the CDC's infographic resembles the 2018-vintage NPC (non-player character) meme [*4]. The beads of sweat illustrated next to the explanation of side effects are a nice touch. The side effects are "signs the vaccine is working." What happens if one doesn't feel side effects? Does that mean the vaccine isn't working? What is the methodology for determining if the vaccine is "working" in the recipient?
In the above screen-shot taken from the CDC's explanation page on viral-vector vaccines [*5], the woman looks distinctly happier compared to the one in the prior-referenced infographic.
No COVID-19 virus is used in the viral-vector vaccine. Instead, a "different, harmless virus" is injected and reprograms cells to produce "spike proteins" that are "only found on the surface of the virus that causes COVID-19." This, ostensibly, stimulates the immune system into producing antibodies and "activating other immune cells to fight off what [the body] thinks is an infection." The goal is for our bodies to learn "how to protect us against future infection with the virus that causes COVID-19." In the mean time, any "temporary discomfort" is assumed as "an indication that the vaccine is working." How long is "temporary?"
The second kind of COVID-19 vaccine is the mRNA (messenger RNA) variety, commonly attributed to the Pfizer and Moderna brands. The CDC states the mRNA vaccines do not contain "ANY virus," [*6] and, again, uses an infographic with an uncanny resemblance to the NPC meme [*7], featuring more beads of sweat pouring down into another explanation of side effects.
Messenger RNA (mRNA) is injected into the body's muscle cells in the upper arm and instructs the creation of spike proteins on the surface of cells, triggering an immune response and "making antibodies, like what happens in natural infection against COVID-19." Prior to injection, the mRNA is "wrapped in a coating that makes delivery easy and keeps the body from damaging it" after injection.
The key to both methods of vaccination involves production of spike proteins on cells to fool the body into inducing an immune response that the body will, ostensibly, memorize and use in case it comes across a genuine COVID-19 virus in the future. This might explain why the vaccines were never tested on human-to-human transmission, since, unlike how vaccines are traditionally created, a dead or weakened sample of the actual the virus isn't used, and the body's means of "learning" to defend against COVID-19 is indirect and vaguely explained. Thus, a more-apt label for these so-called "vaccines" might be "immune-system stimulation products."
How long does the stimulation (or "immunity") last compared to the old-fashioned vaccines that were more-permanent solutions [*8]? All the COVID-19 vaccines rely on production of these "spike proteins." Are the spike proteins themselves harmful? If so, how long do they remain in our bodies? Where do they travel in the body? Can they congregate on certain organs and cause damage?
An article by Dr. Joseph Mercola summarizes findings by Dr. Byram Bridle, a viral immunologist and associate professor at the University of Guelph, Ontario, on the dangers of the spike protein [*9]:
Assuming that the spike protein would not enter into the circulatory system was a “grave mistake,” according to Bridle, who calls the Japanese data “clear-cut evidence” that the vaccine, and the spike protein produced by it, enters your bloodstream and accumulates in vital organs. Bridle also cites recent research showing the spike protein remained in the bloodstream of humans for 29 days.Once in your blood circulation, the spike protein binds to platelet receptors and the cells that line your blood vessels. As explained by Bridle, when that happens, one of several things can occur:It can cause platelets to clump together — Platelets, aka thrombocytes, are specialized cells in your blood that stop bleeding. When there’s blood vessel damage, they clump together to form a blood clot. This is why we’ve been seeing clotting disorders associated with both COVID-19 and the vaccines.It can cause abnormal bleeding. In your heart, it can cause heart problems. In your brain, it can cause neurological damage.Importantly, people who have been vaccinated against COVID-19 absolutely should not donate blood, seeing how the vaccine and the spike protein are both transferred. In fragile patients receiving the blood, the damage could be lethal.Breastfeeding women also need to know that both the vaccine and the spike protein are being expelled in breast milk, and this could be lethal for their babies. You are not transferring antibodies. You are transferring the vaccine itself, as well as the spike protein, which could result in bleeding and/or blood clots in your child. All of this also suggests that for individuals who are at low risk for COVID-19, children and teens in particular, the risks of these vaccines far outweigh the benefits.
Another concern, this one specific to the mRNA vaccines, lies in the casings the mRNA instructions are wrapped in, lipid nanoparticles (LNP). In Dr. Joseph Mercola's May-2020 book, The Truth About COVID-19, at page 132 [*10], he quotes a 2017 article in STAT News, by Damian Garde, critiquing Moderna's casing for mRNA technology [*11]:
In order to protect mRNA molecules from the body’s natural defenses, drug developers must wrap them in a protective casing. For Moderna, that meant putting its Crigler-Najjar therapy in nanoparticles made of lipids. And for its chemists, those nanoparticles created a daunting challenge: Dose too little, and you don’t get enough enzyme to affect the disease; dose too much, and the drug is too toxic for patients.
From the start, Moderna’s scientists knew that using mRNA to spur protein production would be a tough task, so they scoured the medical literature for diseases that might be treated with just small amounts of additional protein.“And that list of diseases is very, very short,” said the former employee … Crigler-Najjar was the lowest-hanging fruit.
Ostensibly, the goldilocks-zone for the right type of casing has now been found. But adverse reactions in some COVID-19 vaccine recipients might be explained by toxicity from the casings or LNPs.Yet Moderna could not make its therapy work … The safe dose was too weak, and repeat injections of a dose strong enough to be effective had troubling effects on the liver in animal studies.
Another concern. How long are the antibodies and "other immune cells" responding to the spike proteins activated for? If activated for too long, can this cause damage? Can COVID-19-vaccine recipients become antibody-dependent? Can this cause more-extensive suffering when recipients are infected with future iterations of corona viruses (i.e. the flu or the common cold)?
Virus antibody dependent enhancement (ADE), as Dr. James Odell explains [*12],
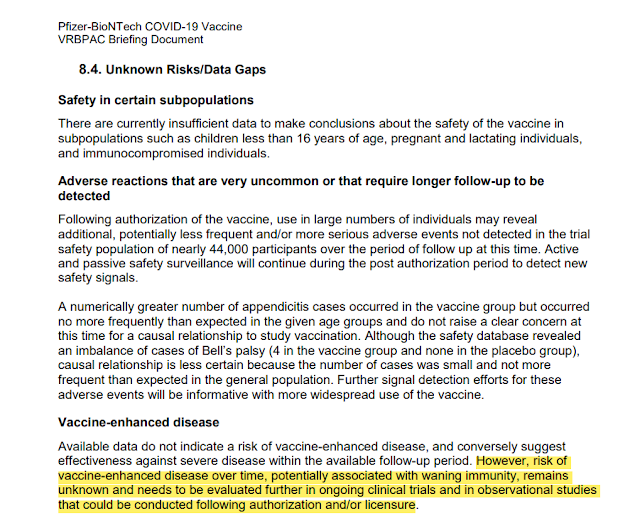
... is a biochemical mechanism in which virus-specific antibodies (usually from a vaccine) promote the entry and/or the replication of another virus into white cells such as monocytes/macrophages and granulocytic cells. This then modulates an overly strong immune response (abnormally enhances it) and induces chronic inflammation, lymphopenia, and/or a ‘cytokine storm’, one or more of which have been reported to cause severe illness and even death. Essentially, ADE is a disease dissemination cycle causing individuals with secondary infection to be more immunologically upregulated than during their first infection (or prior vaccination) by a different strain....In Pfizer's briefing document submitted to the FDA on their COVID-19 vaccine, at page 49 [*13], it admitted that risk of ADE from their COVID-19 vaccine "remains unknown and needs to be evaluated further."
How would we know if ADE is a problem with the COVID-19 vaccines? If mutations of COVID-19, like the alleged "delta variant," cause the COVID-19-vaccinated to become more ill than the unvaccinated compared to the original COVID-19 virus, ADE would be confirmed. What evidence do we have of this so far? ABC reported on July 30, 2021 [*54]:Coronavirus vaccine development began after three SARS epidemics had broken out, starting in early 2002. The Chinese, the Americans, the Europeans all got together and said, “We need to develop a vaccine against coronavirus.” Around 2012, they had about 30 vaccines that looked promising.They took the four best of those and manufactured the vaccines. They gave those vaccines to ferrets, which are the closest analogy when you’re looking at lung infections in human beings.The ferrets had an extraordinarily good antibody response, and that is the metric by which FDA licenses vaccines. So they thought, “We hit the jackpot.” All four of these vaccines worked like a charm. Then something terrible happened. Those ferrets were then exposed to the wild virus, developed inflammation in all their organs, their lungs stopped functioning.The scientists remembered that the same thing had happened in the 1960s when they tried to develop an RSV vaccine, which is an upper respiratory illness very similar to coronavirus. At the time, they did not test it on animals.They went right to human testing. They tested it on about 35 children, and the same thing happened. The children developed a champion antibody response, robust, durable. It looked perfect, and then the children were exposed to the wild virus and they all became sick. Two of them died. They abandoned the vaccine. It was a big embarrassment to FDA and NIH.Those scientists in 2012 remembered that, so, they looked closer and they realized that there are two kinds of antibodies being produced by the coronavirus. There are neutralizing antibodies, which are the kind you want, which fight the disease, and then there are binding antibodies.The binding antibodies actually create a pathway for the disease in your body, and they trigger something called a paradoxical immune response or paradoxical immune enhancement. What that means is that it looks good until you get the disease, and then it makes the disease much, much worse.
As of Thursday, 882 people were tied to the Provincetown outbreak. Among those living in Massachusetts, 74% of them were fully immunized, yet officials said the vast majority were also reporting symptoms. Seven people were reported hospitalized.
You never see the makers, like Pfizer, air television commercials advertising their COVID-19 vaccines. Might regulations requiring a discussion of side effects in the commercials play into that? Why advertise when government is buying the product and giving it away for free, and journalists are advertising your product 24/7 on television with no regulation requiring a discussion of side effects?
You'll often hear from journalists and "fact-checkers" how extremely rare side effects occur in the COVID-19 vaccines. But side effects like "mild fever, headache, and chills" are common, a sign the vaccine is working, and we should presumably tough them out for the greater good. Thus, journalists really mean serious side effects, like being unable to work or perform daily activities (or dying), are rare.
Dr. Mercola estimates an initial serious-side-effect rate of 2.79 percent [*17]:
According to a report by the US Centers for Disease Control and Prevention [CDC], by December 18, 2020, 112,807 Americans had received their first dose of COVID-19 vaccine. Of those, 3,150 suffered one or more “health impact events,” defined as being “unable to perform normal daily activities, unable to work, required care from doctor or health care professional.” That gives us a side effect rate of 2.79 percent.Extrapolated to the total US population of 328.2 million, we may then expect more than 9,156,000 Americans to be injured by the vaccine if every single man, woman, and child is vaccinated. Extrapolated across the global population, the harm will be truly mind-boggling.
COVID-19 vaccine side-effects are reported to the CDC's Vaccine Adverse Event Reporting System (VAERS). I have an analysis, usually updated weekly, that you can read here [*18], as the CDC publishes updated VAERS data every Friday.
The CDC reminds us that just because a report is made doesn't mean the vaccine definitively "caused" an alleged death, permanent disability, or injury. But, designation of COVID on a death certificate requires mere speculation, and no positive PCR test of the decedent is needed (or, if PCR positive, any actual cause of death equals a COVID death); whereas VAERS reporting is voluntary and might account for as little as one percent of actual adverse effects occurring [*19]. Thus, COVID deaths are undoubtedly over-reported and vaccine deaths on VAERS are undoubtedly under-reported. The only question is: to what degree?
The CDC, surprisingly, accepts reports from around the world. About half of the reports come outside the U.S. Here's a screenshot of the current tallies reported for injuries and deaths from the COVID-19 vaccines, as of July 30, 2021 for ALL areas. Click this link to check the data yourself [*20].

So far, that's 11,940 deaths, 12,808 permanent disabilities, and 40,991 hospitalizations out of 573,856 incidents. If those numbers represent one percent of the actual incidents, the true alleged world-wide death count would be 1,194,000.
CDC VAERS tracks data from 1990 to present. A search for any vaccine-related reports ever since 1990, searched on July 30, 2021 yields 20,791 deaths, 32,181 permanent disabilities, and 118,555 hospitalizations out of 1,445,272 incidents. Thus, the COVID-19 vaccines, which were first available in December of 2020, represent 57.43% of all deaths, 39.87% of all permanent disabilities, and 39.71% of all incidents ever reported to VAERS since 1990. The ratios are similar for U.S.-only data (and analyzed here [*21]). That's over half of all vaccine-related deaths attributed to COVID-19 vaccines, despite being available for less than a year, compared to 30 years of data.
The individual VAERS reports can be clicked on and read, unlike COVID-19 death reports. Medicare and Medicaid in the U.S. pay hospitals $13,000 for any COVID-19 patient (and $39,000 if the patient is put on a ventilator) [*22]. Note the rush to attribute any cause of death to COVID-19 as opposed to implicating the vaccine, reported in VAERS ID 1458628-1 for this 35-year-old male, who received one dose of the Pfizer COVID-19 vaccine on April 17, was hospitalized four days later, and died on May 2, 2021:
My previously healthy brother received the Pfizer vaccine (1st dose) and 4 days after he was hospitalized with shortness of breath, heart failure, blood clots in his arm, lungs and leg along with a stroke and many medical conditions kept arising as he was hospitalized. He was in the CICU for a week and a half. Unfortunately, my brother passed away from the Pfizer vaccine. Until his last day the doctors still ""didn't know"" what was wrong with him. A lot happened during his hospital stay, but this is just a brief statement. They have been keeping his medical records from me. They tested him repeatedly there from covid and he wa salways [sic] negative. They had no other explanation to what was happening and all along they wanted it to be COVID-19 and were so quick to say it was not the vaccine.Fact-checkers stress that a report of a death doesn't mean "causation." But what is the goal post for causation? In VAERS ID: 1440769-1, an otherwise-young-and-healthy 28-year-old male got his second Pfizer COVID-19 vaccine dose on May 13, 2021 and died on May 28:
Patient was gone out for a run on 28th May. While running, he collapsed suddenly. Onlookers called 911 and they tried to revive him but he died on the spot. his autopsy result is still pending. He had no history of any illness and had been a healthy individual. He used to exercise regularly. He had received his second dose of vaccine that month on 13th May and had faced expected symptoms like fever and chills that only lasted for 2 days.Try telling this man, who lost his 30-year-old wife four days after receiving the Pfizer COVID-19 vaccine that he's over-reacting, and his wife probably died of a spontaneous heart attack, VAERS ID 1450252-1: "my wife died of a hart attack 4 days after her shot she was only 30 years old,. with no previous symtoms. please explain to me how this could happen [sic]."
Try telling this pilot who lost his 28-year-old wife fifteen days after her first dose of the Moderna COVID-19 vaccine that she died of anorexia and a previous heart condition, completely unrelated to the vaccine, VAERS ID 1243832-1:
4.21.2021- I spoke with (patient's husband) related to spouse. Husband stated the patient has a history of 2nd Degree Type 2 heart block, pacemaker placed at the age of 14, and she currently has issues with an eating disorder dx with anorexia. Patient is reported to be approximately 68-70 pounds at the time of vaccination. March 8.2021- Husband states he and his wife came to receive the vaccine around 1630. After, receiving the vaccine the patient stated to her Husband ""my arm really hurts."" She begin experiencing s/s at approximately 1900 including: fever, chills, runny nose, fatigued and tired - reportedly temperature was 100.0 and the patient began to drink Gatorade and take Tylenol. Monday, 3.15.2021 patient continued to have symptoms therefore, (husband) contacted Moderna Representatives from the safety team, to determine if it would be safe for the patient to get the 2nd vaccine dose - advised everyone that does not have contraindications should be vaccinated-advised to reach out to PCP. Husband stated that the patient did not want to go to her PCP because of her eating disorder. The patient worked from bed during the week per the husband and spent 90-95% of her time in the bed after receiving the vaccine. Husband states on Saturday 3.20.2021 the patients fever had subsided however, she continued to feel poorly and remained bedbound most of the time. Husband is an Pilot 3.23.2021 stated once, he had landed he began trying to contact wife but she was not answering the phone, after several attempts to contact wife - Husband called a neighbor to check on wife. Upon, entering the residence the neighbor found wife lying on the floor unconscious and not breathing. The neighbor notified Husband and called 911. EMS arrived at the scene and pronounced the patient as a DOA. Husband states that the death certification list cardiac arrest, electrolyte imbalance, and heart block, as causes for death. Husband is concerned that the vaccine may have contributed in some way demise of his wife as he stated ""she was never the same after the vaccination.""
This is a spontaneous report from a non-contactable consumer via a regulatory authority. A 33-year-old patient of an unspecified gender received bnt162b2 (BNT162B2), via an unspecified route of administration on an unspecified date at a single dose for covid-19 immunisation. ... The clinical course was as follows: the patient was a pilot who had been vaccinated with bnt162b2. A strong headache occurred immediately after starting the flight. Two hours later, the patient almost lost consciousness and made an emergency landing. (withheld) inoculated and killed three pilots. It's been a fuss, but it doesn't stop anymore. The patient did not know when it will fall when the patient flies (as reported). The clinical outcome of the events, lost consciousness and headache, was unknown. The clinical outcome of the event, death, was fatal....What does "(withheld) inoculated and killed three pilots" mean?
Note this pilot who claims he was permanently disabled from the Pfizer COVID-19 vaccine he took in February 2021, VAERS ID 1026783-1:
I noticed a headache in the very top of my head within an hour of getting the vaccine. I thought it was normal because everyone I know said they got a headache from it. Over the next few hours, the pain moved down the back of my neck and became a burning sensation at the bottom of my skull. The pain was not excruciating but was constant. I thought it would eventually go away. I'm a pilot and fly for a living. Two days after receiving the vaccine I flew my plane and immediately noticed something was wrong with me. I was having a very hard time focusing. Approximately 2 hours into my flying I felt sudden and extreme pressure in my head and nearly blacked out. I immediately landed and stopped flying. Two days later I tried flying again and the exact same thing happened again after 20 minutes. The burning in my neck intensified and was now accompanied by dizziness, nausea, disorientation, confusion, uncontrollable shaking, and tinkling in my toes and fingers. I immediately went to my hometown doctor and he diagnosed me with vertigo. He prescribed me meclizine on Friday 02/05/2021. I took the medicine as prescribed all weekend with no relief. Monday 02/08/2021 I made an appointment for that Wednesday at the Institute. During Wednesday 02/10/2021-02/11/2021 I had roughly 10-15 test performed on me including balance, eye and hearing test, CT scan, MRI, and measured my spinal fluid pressure. The physician determined on 02/11/2021 that I had an allergic reaction to the Pfizer COVID vaccine the severely increased the pressure in my spinal cord and brain stem. That pressure causes my vision problems and ultimately ruptured my left inner ear breaking off several crystals in the process. I cannot fly with this condition....Earlier, I referenced Dr. Mercola analyzing Dr. Bridle's findings regarding transmission of the spike proteins during breastfeeding from COVID-19-vaccinated mothers and his conversation with Robert F. Kennedy on LNP liver-damage in animal studies. As of July 30, 2021, 72 COVID-19-vaccine infant incidents (6-months or younger) are reported on VAERS. Most of these entail transmission through breastfeeding. One is a death report, mother who lost her baby after breastfeeding one day after receiving her second Pfizer COVID-19 vaccine dose, VAERS ID: 1166062-1:
Patient received second dose of Pfizer vaccine on March 17, 2020 while at work. March 18, 2020 her 5 month old breastfed infant developed a rash and within 24 hours was inconsolable, refusing to eat, and developed a fever. Patient brought baby to local ER where assessments were performed, blood analysis revealed elevated liver enzymes. Infant was hospitalized but continued to decline and passed away. Diagnosis of TTP. No known allergies. No new exposures aside from the mother's vaccination the previous day.As discussed earlier, the CDC is concerned with heart inflammation in young men, as a "rare" mRNA COVID-19 vaccine side-effect. Why is the concern limited to "young men?" A search for those COVID-19 vaccine side-effects related to the heart in VAERS reveals few reports among young men, but many among older men and women. For example, VAERS ID 1308944-1 references a 49-year-old female suffering a permanent disability from an enlarged heart two days after her first Moderna COVID-19 vaccine. Perhaps young men are singled out, because, in them, it's harder to pin enlarged heart muscles on alternate causes.
I could go on, but, I invite you to explore the VAERS data for yourself and report your findings instead. I'll leave you with a personal story to consider. In High School, I noticed blood in my urine following a football injury. After an MRI scan of my body, it was discovered I only had one kidney. I was shocked. I assumed that, at birth, doctors would somehow just know I had one kidney and tell me. But how could they have known? It's not like they take inventories of organs at each birth. If it weren't for my football injury, I'd probably go my whole life believing I have two kidneys. It took a specific MRI to reveal I was born with one.
With COVID-19 vaccine injuries, there are the seen and the unseen. After a COVID-19 vaccination, or repeated ones, if continuous revaccination is required, what might you discover later in life that you aren't noticing now when you're younger and healthier?
#4 Immunity for Them, Not for You
 |
| Support this meme's maker, Jimbob, and subscribe here: (arkhavencomics.com) |
For the hundreds of thousands of people around the world with reported adverse effects from COVID-19 vaccines to the U.S. Centers for Disease Control and Prevention's (CDC) Vaccine Adverse Event Reporting System (VAERS) [*1], which may be as low as 1% of the actual victims experiencing adverse effects [*2], and others who are experiencing but not reporting such effects, who's going to pay for their lost wages, physical therapy, drugs, and other resulting needs?
For the over-sixteen-thousand with permanent disabilities from the COVID-19 vaccines reported on VAERS, who's going to pay for the lifetime of care required and compensate them for their pain and suffering? For the over-twelve-thousand reported on VAERS as dead from COVID-19 vaccines, who will compensate their loved ones for their losses?
Making those who made drugs that harmed people pay has traditionally been handled under civil law. Most countries' civil legal systems take their cues from the U.S. and U.K.'s "common law" systems, as judges who've heard cases with particular circumstances write "opinions" based on other judges' "opinions" over hundreds of years. Simply put: (1) someone claims another doing X is wrong and caused harm; (2) a judge explains why X is or isn't wrong, and (3) all future judges conclude similar things to X are wrong or not wrong by referencing what the prior judge said, which is now "law."
Countries without a "common law" system will often copy the opinions of these judges through executive/administrative decree or law by legislatures. Hence, laws around the world aren't exactly uniform, but they are fairly similar.
The subset of civil law that applies to drugs injuring people, "product liability," varies somewhat between jurisdictions, but mostly copies an academic publication titled The Second Restatement of Torts at § 402A, which states [*3]:
Special Liability Of Seller Of Product For Physical Harm To User Or Consumer(1) One who sells any product in a defective condition unreasonably dangerous to the user or consumer or to his property is subject to liability for physical harm thereby caused to the ultimate user or consumer, or to his property, if(a) the seller is engaged in the business of selling such a product, and(b) it is expected to and does reach the user or consumer without substantial change in the condition in which it is sold.(2) The rule stated in Subsection (1) applies although(a) the seller has exercised all possible care in the preparation and sale of his product, and(b) the user or consumer has not bought the product from or entered into any contractual relation with the seller.
A drug company that sells a defective drug, unreasonably dangerous, will pay for any damage its creation causes to the person harmed by it, even if the drug company took the utmost care in creating the drug. Defect can mean the drug could have been designed better but wasn't (defective design), a mistake was made in making the drug by deviating from design (defective manufacture), and/or insufficient safety instructions were provided for the product (defective warning).
To ensure everyone adversely affected by a drug is fairly compensated, victims in most countries can bring claims in "classes," and a drug maker will be forced to pay the entire class. By law, those who might have experienced adverse effects are given notice and an opportunity to "join" a "class action" lawsuit. Thus, one dealing with mildly-irritating side effects who normally wouldn't be bothered to hire a lawyer and sue individually may opt to sign on or be motivated to hire his own lawyer and bring a separate lawsuit. This chain of events from class actions often compounds the amount of money drug-makers would normally pay if class actions weren't allowed.
In the U.S., and other countries, a jury can decide if the drug was defective and, also, how much money to award the injured, which can result in multi-million or even multi-billion-dollar awards that drug makers have to pay. This is why caps on the amount a jury can award are sometimes imposed by legislatures (damage caps), with some controversy [*4].
Imposing damage caps is a priority for makers of drugs that will inherently injure some people. To make a drug that won't injure anyone, (1) all human bodies' reactions to the drug would have to be roughly uniform (which isn't so) or (2) the drug must be given only to a subset of people who will react appropriately to it. A vaccine is, generally, a one-size-fits-all product, but we are different "sizes" regarding our reactions to it, and no one-size-fit-all truly fits all. Your doctor doesn't usually pick a vaccine tailored to your unique body and medical circumstances; he either recommends it for you or he doesn't.
Alas, some people will almost certainly be injured from a vaccine given to the masses. And try arguing to a judge or jury that those injured should suffer without compensation, because the vaccine was "reasonably dangerous." Thus, if a maker can't escape liability, the next best thing is limiting the amount of money it'd be required to pay out and, perhaps more importantly, to prohibit class actions.
The National Childhood Vaccine Injury Act of 1986 (NCVIA), in the U.S., did just that. Ostensibly, drug makers were pulling out of the vaccine market, because the cost of liability insurance was too high for vaccines to be profitable. Congress feared a vaccine shortage and barred the public from suing drug companies over adverse effects from vaccines. It, instead, set up a compensation system through the Federal Court of Claims (colloquially referred to as "Vaccine Court"), a non-jury administrative system that does not allow class actions.
An excise tax is placed of, currently, $0.75 [*5] on each vaccine, and for each disease its designed for, to fund a pool of money to award the injured. Those seeking compensation aren't suing the drug makers but, instead, the U.S. government. Presently, damages are capped at a max of $250,000 (for death). Awards focus on the cost of managing the condition of the injured, ensuring they have funds to pay for their care.
An administrative-law judge (ALJ) in Vaccine Court decides if the vaccine given caused side effects on an "injury table" within a certain period of time. Rather than require mounds of independent medical evidence (which doctors often charge $1,000+/hour to produce), the burden of proof is lower.
The injury table for the seasonal influenza vaccine was last updated in 2017 [*6]. 
The middle box shows the adverse effects the ALJ will consider. The far-right box shows the time-frame the ALJ must find the adverse effects to have materialized within in order to award compensation. For example, did a person develop Guillain-Barré Syndrome ("a rare neurological disorder in which the body's immune system mistakenly attacks part of its peripheral nervous system") [*7] no sooner than three days and no later than 42 days after getting a seasonal influenza vaccine? If so, the ALJ can give an award if a claim in Vaccine Court is filed.
An ALJ can decide if a non-boxed side-effect caused harm, but this would require additional evidence to persuade him. If the ALJ denies a claim, that's it. Design defects are barred from being heard by a jury in the traditional U.S. court system.
This scheme was challenged in the U.S. Supreme Court Case Bruesetwitz v. Wyeth, 562 U.S. 223 (2011) [*8]. The opinion is twenty-eight pages of debate and a ruling in regards to what the following paragraph in the NCVIA means:
No vaccine manufacturer shall be liable in a civil action for damages arising from a vaccine-related injury or death associated with the administration of a vaccine after October 1, 1988, if the injury or death resulted from side effects that were unavoidable even though the vaccine was properly prepared and was accompanied by proper directions and warnings.
Note "properly prepared" refers to defective manufacture and "accompanied by proper directions and warnings" refers to defective warning, two of three aspects of product liability mentioned earlier. Does the phrase "unavoidable" refer to the third aspect, defective design? If so, then the NCVIA wouldn't bar any claims in regular court.
The majority reasoned that defective design claims must be barred, because drug makers wouldn't get anything in exchange for the public having access to what the majority referred to as a "generous" liability and payment scheme in Vaccine Court. Ostensibly, drug makers are "paying" for their immunity from $250,000+ jury awards and class actions via Congress imposing a $0.75 tax on their products that might cut into profits by raising the prices of their vaccines.
In reality, drug makers get two benefits and zero cost from the NCVIA. First, they get immunity from liability in the traditional court system. Second, they avoid defending themselves in Vaccine Court (as the U.S. government handles the claims for injury) and defer any compensation to the injured through a, currently, $0.75 tax on each vaccine given.
This liability scheme was designed to encourage drug makers to produce vaccines so there won't be shortages. Legislatures and administrative agencies can't create medical remedies for novel disease out of thin air; they rely on the private sector to produce remedies for the public. The U.S. Congress, and others around the world, thought ahead: what if a medical emergency necessitated rapid distribution of a medical remedy?
Thus, in 2005, a new U.S. law, the Public Readiness and Emergency Preparedness Act (PREP Act), which authorizes the Department of Health and Human Services (HHS) to declare even more immunity from liability for any claims related to "emergency countermeasure" vaccines and any other countermeasures (like drugs and medical devices) "against diseases or other threats of public health emergencies" [*9], was enacted, inspiring governments around the world to mirror it.
Law can put people in jail. It can tax people. But it can't produce a remedy for a public-health emergency. Normally, makers of remedies could be sued under product-liability laws if they try to remedy a health emergency and wind up harming people, meaning their failure could bankrupt them in legal fees, insurance costs, and judgment-awards they'd owe. But, if vaccine makers were given an additional boost in legal immunity, beyond the NCVIA, perhaps their ingenuity could be stimulated to produce remedies to public-health emergencies.
First, a "countermeasure," like a vaccine, is approved by the jurisdiction's regulatory agency for "emergency use." Normally, regulatory agencies like, in the U.S., the Food and Drug Administration (FDA), require many months of testing of long-term health risks for vaccines before approving them for general use. But, the regulatory demands for testing are severely truncated for what are redeemed as "emergency countermeasures" by the HHS. This truncated "testing," in the U.S., for COVID-19 vaccines as an emergency countermeasure was thoroughly discussed in part 2 (of 4) of this piece that you can read here [*10].
Once approved as an emergency countermeasure, an absurd level of liability protection is afforded. This is where the rabbit-hole we're about to enter begets a truly wild ride. Note the HHS's enactment and interpretation of liability protection for COVID-19 vaccines as an emergency countermeasure [*11]. 
Absent "willful misconduct," meaning the vaccine maker intentionally tried to injure people or acted with reckless disregard for whether they would or wouldn't injure people, no claims can be brought in the regular, judicial, U.S. court system.
Immunity from litigation extends not only to the COVID-19 vaccine makers, but any person or entity participating in the distribution of the product. As long as someone is injured in an event with "a direct connection to [a] countermeasure's administration or use," he/she or it is immune from litigation. Thus, immunity from liability goes far beyond mere design defects.
If a vaccine delivery truck runs over and kills people on its vaccination-site delivery path, the victims, according to the HHS, aren't allowed to sue. If, in the course of injecting one with the vaccine, someone slips and falls, the injured have no right to sue, since the slip and fall resulted from the attempt to give a "covered countermeasure."
Can victims, nonetheless, bring claims in Vaccine Court? Ostensibly, yes. But, good luck proving your claim [*12].
Claim against those using an HHS-approved countermeasure (like the COVID-19 vaccines) must be "supported by compelling, reliable, valid, medical and scientific evidence." In law, "compelling" means beyond the normal suing-people standard of "preponderance of the evidence." Further, the word "and" is critical here. Scientific evidence requires long-term studies into the side effects. Emergency-use authorization negates such studies. So, how is one to prove with "scientific evidence" that his/her injury is related to a COVID-19 vaccine?
As long as COVID-19 vaccines remain under "emergency use" provisions of the PREP Act, or under similar schemes in other countries, it is effectively impossible to bring a successful claim without additional studies.
Hopefully, future studies on the harmful effects of the COVID-19 vaccines, as discussed in part 3 (of 4) of this series here [*13], will allow such claims to be brought.
Eventually, I believe such evidence will come to light. Then, a tsunami of claims will be brought. Thus, lawyers might want to research and practice their skills in this area to assist if and when the time for justice is ripe.
---
FOOTNOTES
Part #1: If the COVID-19 Vaccines Are Dangerous, How Come the Media Isn't Telling Us?
[*1] https://www.yahoo.com/news/biden-working-ensure-u-booster-011541467.html
[*2] https://stratagemsoftheright.blogspot.com/2021/04/the-politics-of-masks-virtuous.html
[*3] https://stratagemsoftheright.blogspot.com/2021/04/to-get-or-not-get-not-vaccine-anatomy.html
[*4] https://stratagemsoftheright.blogspot.com/2021/05/covid-19-not-vaccines-represent-41-of.html
[*5] https://wonder.cdc.gov/vaers.html
[*6] https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
[*7] Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (p. xiv). Chelsea Green Publishing. Kindle Edition. https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY
[*8] https://www.washingtonpost.com/technology/2020/03/03/facebook-pharma-ads/
[*9] https://www.cnbc.com/2020/06/30/chobani-pfizer-and-sap-join-list-of-companies-pulling-faebook-ad-spend.html
[*10] https://www.projectveritas.com/news/breaking-facebook-whistleblowers-expose-leaked-internal-docs-detailing-new/
[*11] https://www.reuters.com/article/uk-factcheck-transmission-idUSKBN29N1UH
[*12] https://stratagemsoftheright.blogspot.com/2021/04/to-get-or-not-get-not-vaccine-anatomy.html
[*13] https://stratagemsoftheright.blogspot.com/2021/02/evidence-in-long-shadow-of-civilization.html
[*14] https://archive.is/xLGE5#selection-181.208-181.247
[*15] https://advances.sciencemag.org/content/7/21/eabd1705
Science Advances 21 May 2021: Vol. 7, no. 21, eabd1705 DOI: 10.1126/sciadv.abd1705
[*1] https://www.bmj.com/content/371/bmj.m4037
[*2] https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19
[*3] https://www.nature.com/articles/d41586-020-03219-y
[*4] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (pp. 78-79). Chelsea Green Publishing. Kindle Edition.
[*5] https://link.springer.com/article/10.1007/s10096-020-03913-9
[*6] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (p. 77). Chelsea Green Publishing. Kindle Edition.
[*7] https://stratagemsoftheright.blogspot.com/2021/01/the-broken-thumb-heuristics-in-fall-of.html
[*8] https://www.fox35orlando.com/news/fox-35-investigates-florida-department-of-health-says-some-labs-have-not-reported-negative-covid-19-results
[*9] https://www.msn.com/en-us/health/medical/half-of-cdc-coronavirus-test-kits-are-inaccurate-study-finds/ar-BB16S6M6
[*10] https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
[*11] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219423/
[*12] https://blogs.bmj.com/bmj/2020/11/26/peter-doshi-pfizer-and-modernas-95-effective-vaccines-lets-be-cautious-and-first-see-the-full-data/
[*13] https://www.modernatx.com/sites/default/files/mRNA-1273-P301-Protocol.pdf
[*14] https://mises.org/wire/what-covid-vaccine-hype-fails-mention
[*15] Id.
[*18] https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html
[*19] https://stratagemsoftheright.blogspot.com/2021/04/the-politics-of-masks-virtuous.html
[*20] https://www.bmj.com/content/371/bmj.m4037
[*21] Id.
[*22] Id.
Part #3: Adverse Effects: the Seen and the Unseen
[*1] Yes, I'm aware "counter-effective" isn't technically a word. But if a vaccine causes the body to allow more damage from a future iteration of a virus, it would be not just ineffective but, also, bringing about the opposite of the intended result. Dr. Robert Malone's discussion with Steve Bannon can be viewed here: https://rumble.com/vkfz1v-the-vaccine-causes-the-virus-to-be-more-dangerous.html
[*2] https://www.cdc.gov/vaccines/covid-19/clinical-considerations/myocarditis.html
[*3] https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/viralvector.html
[*4] https://www.cdc.gov/coronavirus/2019-ncov/downloads/vaccines/COVID-19-viral-vector-infographic_D_FINAL-508_030621.pdf
[*5] https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/viralvector.html
[*6] https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html
[*7] https://www.cdc.gov/coronavirus/2019-ncov/downloads/vaccines/COVID-19-mRNA-infographic_G_508.pdf
[*8] https://stratagemsoftheright.blogspot.com/2021/04/to-get-or-not-get-not-vaccine-anatomy.html
[*9] https://openontario.ca/articles/2021/06/23/dr-mercola-explains-dr-bridles-bombshell-revelations-regarding-spike-proteins
[*10] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (p. 132). Chelsea Green Publishing. Kindle Edition.
[*11] https://www.statnews.com/2017/01/10/moderna-trouble-mrna/
[*12] https://www.biologicalmedicineinstitute.com/post/covid-19-mrna-vaccines
[*13] https://www.fda.gov/media/144245/download
[*14] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (pp. 134-135). Chelsea Green Publishing. Kindle Edition.
[*15] https://abc7news.com/cape-cod-covid-outbreak-cdc-mask-guidance-face-masks-delta-variant/10918914/
[*16] https://stratagemsoftheright.blogspot.com/2021/05/what-to-consider-before-getting-covid.html
[*17] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (p. 138). Chelsea Green Publishing. Kindle Edition.
[*18] https://stratagemsoftheright.blogspot.com/2021/05/covid-19-not-vaccines-represent-41-of.html
[*19] https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
[*20] https://wonder.cdc.gov/vaers.html
[*21] https://stratagemsoftheright.blogspot.com/2021/05/covid-19-not-vaccines-represent-41-of.html
[*22] https://www.usatoday.com/story/news/factcheck/2020/04/24/fact-check-medicare-hospitals-paid-more-covid-19-patients-coronavirus/3000638001/
Part #4: Immunity for Them, Not for You
[*1] https://wonder.cdc.gov/vaers.html
[*2] https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
[*3] The Second Restatement of Torts, § 402A https://h2o.law.harvard.edu/text_blocks/134
[*4] The Seventh Amendment of the U.S. Constitution states: "In suits at common law, where the value in controversy shall exceed twenty dollars, the right of trial by jury shall be preserved, and no fact tried by a jury, shall be otherwise reexamined in any court of the United States, than according to the rules of the common law." https://www.law.cornell.edu/constitution/seventh_amendment Argument ensues as to whether a "fact tried by the jury" can also be the award in dollars that would exceed a damage cap imposed by a legislature. Common law is law made by judges, not legislatures. Thus, arguably, only a judge could change a jury award, and damage caps are "unconstitutional."
[*5] The Health Resources and Services Administration in the U.S. states:
Funded by a $.75 excise tax on vaccines recommended by the Centers for Disease Control and Prevention for routine administration to children, the excise tax is imposed on each dose (i.e., disease that is prevented) of a vaccine. Trivalent influenza vaccine for example, is taxed $.75 because it prevents one disease; measles-mumps-rubella vaccine, which prevents three diseases, is taxed $2.25.
https://www.hrsa.gov/vaccine-compensation/about/index.html
[*6] https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/d/injury-table.pdf
[*7] https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Guillain-Barr%C3%A9-Syndrome-Fact-Sheet
[*8] https://www.supremecourt.gov/opinions/10pdf/09-152.pdf
[*9] https://www.hrsa.gov/vaccine-compensation/about/index.html
[*10] https://stratagemsoftheright.blogspot.com/2021/06/false-efficacy-difference-between.html
[*11] https://www.federalregister.gov/documents/2020/03/17/2020-05484/declaration-under-the-public-readiness-and-emergency-preparedness-act-for-medical-countermeasures
[*12] https://www.hrsa.gov/cicp/
[*13] https://stratagemsoftheright.blogspot.com/2021/07/adverse-effects-seen-and-unseen-pt-3-of.html









Comments
Post a Comment