Adverse Effects: the Seen and the Unseen (Pt. 3 of What to Consider Before Getting a COVID-19 "Vaccine" or Semi-Annual Revaxx)
NOTE: Below is part 3 of What to Consider Before Getting a COVID-19 "Vaccine" or Semi-Annual Re-Vaxx. If you haven't read parts 1 and/or 2 yet, you may click the prior-referenced link to read them, which will also include further parts subsequently added.
Part #3 Adverse Effects: the Seen and the Unseen
If the COVID-19 vaccines are less effective than the media proclaims or ineffective (setting aside evidence, as Dr. Robert Malone suggests, that they may be counter-effective via antibody-dependent enhancement [*1]), what's the harm in taking them anyway? Anecdotally, you likely know many people who've taken them and experienced mild side-effects for a day or two that resolved, and some who may have experienced no side effects. If it's free to take one of these emergency-use-authorized vaccines, what have you got to lose by trying one out? How can we measure the societal risk-to-reward ratio in mass COVID-19 vaccination?
Everyone, even those we'd label "pro-vaccine," agrees adverse effects from the COVID-19 vaccines exist. The only questions are: (1) how often, (2) how severe, and (3) for how long? How do we measure these variables? Do severe and/or long-lasting effects kick in only within a few days after receiving a vaccine? Or, can they be seen one month, or, perhaps, years into the future? Years in the future, how would we know if a person is experiencing a health condition (e.g., an enlarged heart muscle, as the U.S. Centers for Disease Control and Prevention (CDC) confesses [*2]) that is causally connected to the vaccine he took years ago? When people say adverse effects are "uncommon," how pervasive must future-reported side effects be before that label would be retracted?
Every day, we learn something new about adverse effects from the COVID-19 vaccines. But, at some point, it's time to pause spectating and start congregating and analyzing information. As of July 30, 2021, here are some critical things we know.
There are two kinds of COVID-19 vaccines being offered. One is the Johnson and Johnson (in the U.S.) and Astrozeneca (in Europe) kind, commonly described as "viral vector" vaccines. Since the world's various organizations tend to take the CDC's word as gospel on the COVID situation, let's see what the CDC proclaims about the viral-vector vaccines [*3].
Notice the CDC's infographic resembles the 2018-vintage NPC (non-player character) meme [*4]. The beads of sweat illustrated next to the explanation of side effects are a nice touch. The side effects are "signs the vaccine is working." What happens if one doesn't feel side effects? Does that mean the vaccine isn't working? What is the methodology for determining if the vaccine is "working" in the recipient?
In the above screen-shot taken from the CDC's explanation page on viral-vector vaccines [*5], the woman looks distinctly happier compared to the one in the prior-referenced infographic.
No COVID-19 virus is used in the viral-vector vaccine. Instead, a "different, harmless virus" is injected and reprograms cells to produce "spike proteins" that are "only found on the surface of the virus that causes COVID-19." This, ostensibly, stimulates the immune system into producing antibodies and "activating other immune cells to fight off what [the body] thinks is an infection." The goal is for our bodies to learn "how to protect us against future infection with the virus that causes COVID-19." In the mean time, any "temporary discomfort" is assumed as "an indication that the vaccine is working." How long is "temporary?"
The second kind of COVID-19 vaccine is the mRNA (messenger RNA) variety, commonly attributed to the Pfizer and Moderna brands. The CDC states the mRNA vaccines do not contain "ANY virus," [*6] and, again, uses an infographic with an uncanny resemblance to the NPC meme [*7], featuring more beads of sweat pouring down into another explanation of side effects.
Messenger RNA (mRNA) is injected into the body's muscle cells in the upper arm and instructs the creation of spike proteins on the surface of cells, triggering an immune response and "making antibodies, like what happens in natural infection against COVID-19." Prior to injection, the mRNA is "wrapped in a coating that makes delivery easy and keeps the body from damaging it" after injection.
The key to both methods of vaccination involves production of spike proteins on cells to fool the body into inducing an immune response that the body will, ostensibly, memorize and use in case it comes across a genuine COVID-19 virus in the future. This might explain why the vaccines were never tested on human-to-human transmission, since, unlike how vaccines are traditionally created, a dead or weakened sample of the actual the virus isn't used, and the body's means of "learning" to defend against COVID-19 is indirect and vaguely explained. Thus, a more-apt label for these so-called "vaccines" might be "immune-system stimulation products."
How long does the stimulation (or "immunity") last compared to the old-fashioned vaccines that were more-permanent solutions [*8]? All the COVID-19 vaccines rely on production of these "spike proteins." Are the spike proteins themselves harmful? If so, how long do they remain in our bodies? Where do they travel in the body? Can they congregate on certain organs and cause damage?
An article by Dr. Joseph Mercola summarizes findings by Dr. Byram Bridle, a viral immunologist and associate professor at the University of Guelph, Ontario, on the dangers of the spike protein [*9]:
Assuming that the spike protein would not enter into the circulatory system was a “grave mistake,” according to Bridle, who calls the Japanese data “clear-cut evidence” that the vaccine, and the spike protein produced by it, enters your bloodstream and accumulates in vital organs. Bridle also cites recent research showing the spike protein remained in the bloodstream of humans for 29 days.Once in your blood circulation, the spike protein binds to platelet receptors and the cells that line your blood vessels. As explained by Bridle, when that happens, one of several things can occur:It can cause platelets to clump together — Platelets, aka thrombocytes, are specialized cells in your blood that stop bleeding. When there’s blood vessel damage, they clump together to form a blood clot. This is why we’ve been seeing clotting disorders associated with both COVID-19 and the vaccines.It can cause abnormal bleeding. In your heart, it can cause heart problems. In your brain, it can cause neurological damage.Importantly, people who have been vaccinated against COVID-19 absolutely should not donate blood, seeing how the vaccine and the spike protein are both transferred. In fragile patients receiving the blood, the damage could be lethal.Breastfeeding women also need to know that both the vaccine and the spike protein are being expelled in breast milk, and this could be lethal for their babies. You are not transferring antibodies. You are transferring the vaccine itself, as well as the spike protein, which could result in bleeding and/or blood clots in your child. All of this also suggests that for individuals who are at low risk for COVID-19, children and teens in particular, the risks of these vaccines far outweigh the benefits.
Another concern, this one specific to the mRNA vaccines, lies in the casings the mRNA instructions are wrapped in, lipid nanoparticles (LNP). In Dr. Joseph Mercola's May-2020 book, The Truth About COVID-19, at page 132 [*10], he quotes a 2017 article in STAT News, by Damian Garde, critiquing Moderna's casing for mRNA technology [*11]:
In order to protect mRNA molecules from the body’s natural defenses, drug developers must wrap them in a protective casing. For Moderna, that meant putting its Crigler-Najjar therapy in nanoparticles made of lipids. And for its chemists, those nanoparticles created a daunting challenge: Dose too little, and you don’t get enough enzyme to affect the disease; dose too much, and the drug is too toxic for patients.
From the start, Moderna’s scientists knew that using mRNA to spur protein production would be a tough task, so they scoured the medical literature for diseases that might be treated with just small amounts of additional protein.
“And that list of diseases is very, very short,” said the former employee … Crigler-Najjar was the lowest-hanging fruit.
Ostensibly, the goldilocks-zone for the right type of casing has now been found. But adverse reactions in some COVID-19 vaccine recipients might be explained by toxicity from the casings or LNPs.Yet Moderna could not make its therapy work … The safe dose was too weak, and repeat injections of a dose strong enough to be effective had troubling effects on the liver in animal studies.
Another concern. How long are the antibodies and "other immune cells" responding to the spike proteins activated for? If activated for too long, can this cause damage? Can COVID-19-vaccine recipients become antibody-dependent? Can this cause more-extensive suffering when recipients are infected with future iterations of corona viruses (i.e. the flu or the common cold)?
Virus antibody dependent enhancement (ADE), as Dr. James Odell explains [*12],
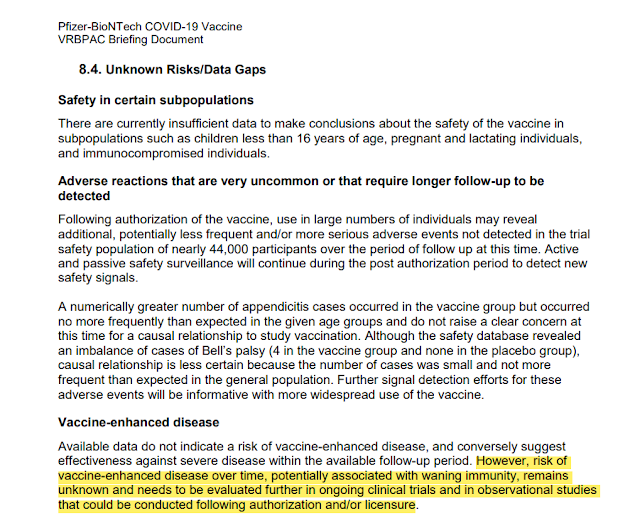
... is a biochemical mechanism in which virus-specific antibodies (usually from a vaccine) promote the entry and/or the replication of another virus into white cells such as monocytes/macrophages and granulocytic cells. This then modulates an overly strong immune response (abnormally enhances it) and induces chronic inflammation, lymphopenia, and/or a ‘cytokine storm’, one or more of which have been reported to cause severe illness and even death. Essentially, ADE is a disease dissemination cycle causing individuals with secondary infection to be more immunologically upregulated than during their first infection (or prior vaccination) by a different strain....In Pfizer's briefing document submitted to the FDA on their COVID-19 vaccine, at page 49 [*13], it admitted that risk of ADE from their COVID-19 vaccine "remains unknown and needs to be evaluated further."
How would we know if ADE is a problem with the COVID-19 vaccines? If mutations of COVID-19, like the alleged "delta variant," cause the COVID-19-vaccinated to become more ill than the unvaccinated compared to the original COVID-19 virus, ADE would be confirmed. What evidence do we have of this so far? ABC reported on July 30, 2021 [*54]:Coronavirus vaccine development began after three SARS epidemics had broken out, starting in early 2002. The Chinese, the Americans, the Europeans all got together and said, “We need to develop a vaccine against coronavirus.” Around 2012, they had about 30 vaccines that looked promising.They took the four best of those and manufactured the vaccines. They gave those vaccines to ferrets, which are the closest analogy when you’re looking at lung infections in human beings.The ferrets had an extraordinarily good antibody response, and that is the metric by which FDA licenses vaccines. So they thought, “We hit the jackpot.” All four of these vaccines worked like a charm. Then something terrible happened. Those ferrets were then exposed to the wild virus, developed inflammation in all their organs, their lungs stopped functioning.The scientists remembered that the same thing had happened in the 1960s when they tried to develop an RSV vaccine, which is an upper respiratory illness very similar to coronavirus. At the time, they did not test it on animals.They went right to human testing. They tested it on about 35 children, and the same thing happened. The children developed a champion antibody response, robust, durable. It looked perfect, and then the children were exposed to the wild virus and they all became sick. Two of them died. They abandoned the vaccine. It was a big embarrassment to FDA and NIH.Those scientists in 2012 remembered that, so, they looked closer and they realized that there are two kinds of antibodies being produced by the coronavirus. There are neutralizing antibodies, which are the kind you want, which fight the disease, and then there are binding antibodies.The binding antibodies actually create a pathway for the disease in your body, and they trigger something called a paradoxical immune response or paradoxical immune enhancement. What that means is that it looks good until you get the disease, and then it makes the disease much, much worse.
As of Thursday, 882 people were tied to the Provincetown outbreak. Among those living in Massachusetts, 74% of them were fully immunized, yet officials said the vast majority were also reporting symptoms. Seven people were reported hospitalized.
You never see the makers, like Pfizer, air television commercials advertising their COVID-19 vaccines. Might regulations requiring a discussion of side effects in the commercials play into that? Why advertise when government is buying the product and giving it away for free, and journalists are advertising your product 24/7 on television with no regulation requiring a discussion of side effects?
You'll often hear from journalists and "fact-checkers" how extremely rare side effects occur in the COVID-19 vaccines. But side effects like "mild fever, headache, and chills" are common, a sign the vaccine is working, and we should presumably tough them out for the greater good. Thus, journalists really mean serious side effects, like being unable to work or perform daily activities (or dying), are rare.
Dr. Mercola estimates an initial serious-side-effect rate of 2.79 percent [*17]:
According to a report by the US Centers for Disease Control and Prevention [CDC], by December 18, 2020, 112,807 Americans had received their first dose of COVID-19 vaccine. Of those, 3,150 suffered one or more “health impact events,” defined as being “unable to perform normal daily activities, unable to work, required care from doctor or health care professional.” That gives us a side effect rate of 2.79 percent.Extrapolated to the total US population of 328.2 million, we may then expect more than 9,156,000 Americans to be injured by the vaccine if every single man, woman, and child is vaccinated. Extrapolated across the global population, the harm will be truly mind-boggling.
COVID-19 vaccine side-effects are reported to the CDC's Vaccine Adverse Event Reporting System (VAERS). I have an analysis, usually updated weekly, that you can read here [*18], as the CDC publishes updated VAERS data every Friday.
The CDC reminds us that just because a report is made doesn't mean the vaccine definitively "caused" an alleged death, permanent disability, or injury. But, designation of COVID on a death certificate requires mere speculation, and no positive PCR test of the decedent is needed (or, if PCR positive, any actual cause of death equals a COVID death); whereas VAERS reporting is voluntary and might account for as little as one percent of actual adverse effects occurring [*19]. Thus, COVID deaths are undoubtedly over-reported and vaccine deaths on VAERS are undoubtedly under-reported. The only question is: to what degree?
The CDC, surprisingly, accepts reports from around the world. About half of the reports come outside the U.S. Here's a screenshot of the current tallies reported for injuries and deaths from the COVID-19 vaccines, as of July 30, 2021 for ALL areas. Click this link to check the data yourself [*20].

So far, that's 11,940 deaths, 12,808 permanent disabilities, and 40,991 hospitalizations out of 573,856 incidents. If those numbers represent one percent of the actual incidents, the true alleged world-wide death count would be 1,194,000.
CDC VAERS tracks data from 1990 to present. A search for any vaccine-related reports ever since 1990, searched on July 30, 2021 yields 20,791 deaths, 32,181 permanent disabilities, and 118,555 hospitalizations out of 1,445,272 incidents. Thus, the COVID-19 vaccines, which were first available in December of 2020, represent 57.43% of all deaths, 39.87% of all permanent disabilities, and 39.71% of all incidents ever reported to VAERS since 1990. The ratios are similar for U.S.-only data (and analyzed here [*21]). That's over half of all vaccine-related deaths attributed to COVID-19 vaccines, despite being available for less than a year, compared to 30 years of data.
The individual VAERS reports can be clicked on and read, unlike COVID-19 death reports. Medicare and Medicaid in the U.S. pay hospitals $13,000 for any COVID-19 patient (and $39,000 if the patient is put on a ventilator) [*22]. Note the rush to attribute any cause of death to COVID-19 as opposed to implicating the vaccine, reported in VAERS ID 1458628-1 for this 35-year-old male, who received one dose of the Pfizer COVID-19 vaccine on April 17, was hospitalized four days later, and died on May 2, 2021:
My previously healthy brother received the Pfizer vaccine (1st dose) and 4 days after he was hospitalized with shortness of breath, heart failure, blood clots in his arm, lungs and leg along with a stroke and many medical conditions kept arising as he was hospitalized. He was in the CICU for a week and a half. Unfortunately, my brother passed away from the Pfizer vaccine. Until his last day the doctors still ""didn't know"" what was wrong with him. A lot happened during his hospital stay, but this is just a brief statement. They have been keeping his medical records from me. They tested him repeatedly there from covid and he wa salways [sic] negative. They had no other explanation to what was happening and all along they wanted it to be COVID-19 and were so quick to say it was not the vaccine.Fact-checkers stress that a report of a death doesn't mean "causation." But what is the goal post for causation? In VAERS ID: 1440769-1, an otherwise-young-and-healthy 28-year-old male got his second Pfizer COVID-19 vaccine dose on May 13, 2021 and died on May 28:
Patient was gone out for a run on 28th May. While running, he collapsed suddenly. Onlookers called 911 and they tried to revive him but he died on the spot. his autopsy result is still pending. He had no history of any illness and had been a healthy individual. He used to exercise regularly. He had received his second dose of vaccine that month on 13th May and had faced expected symptoms like fever and chills that only lasted for 2 days.Try telling this man, who lost his 30-year-old wife four days after receiving the Pfizer COVID-19 vaccine that he's over-reacting, and his wife probably died of a spontaneous heart attack, VAERS ID 1450252-1: "my wife died of a hart attack 4 days after her shot she was only 30 years old,. with no previous symtoms. please explain to me how this could happen [sic]."
Try telling this pilot who lost his 28-year-old wife fifteen days after her first dose of the Moderna COVID-19 vaccine that she died of anorexia and a previous heart condition, completely unrelated to the vaccine, VAERS ID 1243832-1:
4.21.2021- I spoke with (patient's husband) related to spouse. Husband stated the patient has a history of 2nd Degree Type 2 heart block, pacemaker placed at the age of 14, and she currently has issues with an eating disorder dx with anorexia. Patient is reported to be approximately 68-70 pounds at the time of vaccination. March 8.2021- Husband states he and his wife came to receive the vaccine around 1630. After, receiving the vaccine the patient stated to her Husband ""my arm really hurts."" She begin experiencing s/s at approximately 1900 including: fever, chills, runny nose, fatigued and tired - reportedly temperature was 100.0 and the patient began to drink Gatorade and take Tylenol. Monday, 3.15.2021 patient continued to have symptoms therefore, (husband) contacted Moderna Representatives from the safety team, to determine if it would be safe for the patient to get the 2nd vaccine dose - advised everyone that does not have contraindications should be vaccinated-advised to reach out to PCP. Husband stated that the patient did not want to go to her PCP because of her eating disorder. The patient worked from bed during the week per the husband and spent 90-95% of her time in the bed after receiving the vaccine. Husband states on Saturday 3.20.2021 the patients fever had subsided however, she continued to feel poorly and remained bedbound most of the time. Husband is an Pilot 3.23.2021 stated once, he had landed he began trying to contact wife but she was not answering the phone, after several attempts to contact wife - Husband called a neighbor to check on wife. Upon, entering the residence the neighbor found wife lying on the floor unconscious and not breathing. The neighbor notified Husband and called 911. EMS arrived at the scene and pronounced the patient as a DOA. Husband states that the death certification list cardiac arrest, electrolyte imbalance, and heart block, as causes for death. Husband is concerned that the vaccine may have contributed in some way demise of his wife as he stated ""she was never the same after the vaccination.""
This is a spontaneous report from a non-contactable consumer via a regulatory authority. A 33-year-old patient of an unspecified gender received bnt162b2 (BNT162B2), via an unspecified route of administration on an unspecified date at a single dose for covid-19 immunisation. ... The clinical course was as follows: the patient was a pilot who had been vaccinated with bnt162b2. A strong headache occurred immediately after starting the flight. Two hours later, the patient almost lost consciousness and made an emergency landing. (withheld) inoculated and killed three pilots. It's been a fuss, but it doesn't stop anymore. The patient did not know when it will fall when the patient flies (as reported). The clinical outcome of the events, lost consciousness and headache, was unknown. The clinical outcome of the event, death, was fatal....What does "(withheld) inoculated and killed three pilots" mean?
Note this pilot who claims he was permanently disabled from the Pfizer COVID-19 vaccine he took in February 2021, VAERS ID 1026783-1:
I noticed a headache in the very top of my head within an hour of getting the vaccine. I thought it was normal because everyone I know said they got a headache from it. Over the next few hours, the pain moved down the back of my neck and became a burning sensation at the bottom of my skull. The pain was not excruciating but was constant. I thought it would eventually go away. I'm a pilot and fly for a living. Two days after receiving the vaccine I flew my plane and immediately noticed something was wrong with me. I was having a very hard time focusing. Approximately 2 hours into my flying I felt sudden and extreme pressure in my head and nearly blacked out. I immediately landed and stopped flying. Two days later I tried flying again and the exact same thing happened again after 20 minutes. The burning in my neck intensified and was now accompanied by dizziness, nausea, disorientation, confusion, uncontrollable shaking, and tinkling in my toes and fingers. I immediately went to my hometown doctor and he diagnosed me with vertigo. He prescribed me meclizine on Friday 02/05/2021. I took the medicine as prescribed all weekend with no relief. Monday 02/08/2021 I made an appointment for that Wednesday at the Institute. During Wednesday 02/10/2021-02/11/2021 I had roughly 10-15 test performed on me including balance, eye and hearing test, CT scan, MRI, and measured my spinal fluid pressure. The physician determined on 02/11/2021 that I had an allergic reaction to the Pfizer COVID vaccine the severely increased the pressure in my spinal cord and brain stem. That pressure causes my vision problems and ultimately ruptured my left inner ear breaking off several crystals in the process. I cannot fly with this condition....Earlier, I referenced Dr. Mercola analyzing Dr. Bridle's findings regarding transmission of the spike proteins during breastfeeding from COVID-19-vaccinated mothers and his conversation with Robert F. Kennedy on LNP liver-damage in animal studies. As of July 30, 2021, 72 COVID-19-vaccine infant incidents (6-months or younger) are reported on VAERS. Most of these entail transmission through breastfeeding. One is a death report, mother who lost her baby after breastfeeding one day after receiving her second Pfizer COVID-19 vaccine dose, VAERS ID: 1166062-1:
Patient received second dose of Pfizer vaccine on March 17, 2020 while at work. March 18, 2020 her 5 month old breastfed infant developed a rash and within 24 hours was inconsolable, refusing to eat, and developed a fever. Patient brought baby to local ER where assessments were performed, blood analysis revealed elevated liver enzymes. Infant was hospitalized but continued to decline and passed away. Diagnosis of TTP. No known allergies. No new exposures aside from the mother's vaccination the previous day.As discussed earlier, the CDC is concerned with heart inflammation in young men, as a "rare" mRNA COVID-19 vaccine side-effect. Why is the concern limited to "young men?" A search for those COVID-19 vaccine side-effects related to the heart in VAERS reveals few reports among young men, but many among older men and women. For example, VAERS ID 1308944-1 references a 49-year-old female suffering a permanent disability from an enlarged heart two days after her first Moderna COVID-19 vaccine. Perhaps young men are singled out, because, in them, it's harder to pin enlarged heart muscles on alternate causes.
I could go on, but, I invite you to explore the VAERS data for yourself and report your findings instead. I'll leave you with a personal story to consider. In High School, I noticed blood in my urine following a football injury. After an MRI scan of my body, it was discovered I only had one kidney. I was shocked. I assumed that, at birth, doctors would somehow just know I had one kidney and tell me. But how could they have known? It's not like they take inventories of organs at each birth. If it weren't for my football injury, I'd probably go my whole life believing I have two kidneys. It took a specific MRI to reveal I was born with one.
With COVID-19 vaccine injuries, there are the seen and the unseen. After a COVID-19 vaccination, or repeated ones, if continuous revaccination is required, what might you discover later in life that you aren't noticing now when you're younger and healthier?
Continued in Part 4, Immunity for Them, Not for You.
All prior and subsequent parts, as they are published, can be read here.---
FOOTNOTES
[*1] Yes, I'm aware "counter-effective" isn't technically a word. But if a vaccine causes the body to allow more damage from a future iteration of a virus, it would be not just ineffective but, also, bringing about the opposite of the intended result. Dr. Robert Malone's discussion with Steve Bannon can be viewed here: https://rumble.com/vkfz1v-the-vaccine-causes-the-virus-to-be-more-dangerous.html
[*2] https://www.cdc.gov/vaccines/covid-19/clinical-considerations/myocarditis.html
[*3] https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/viralvector.html
[*4] https://www.cdc.gov/coronavirus/2019-ncov/downloads/vaccines/COVID-19-viral-vector-infographic_D_FINAL-508_030621.pdf
[*5] https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/viralvector.html
[*6] https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html
[*7] https://www.cdc.gov/coronavirus/2019-ncov/downloads/vaccines/COVID-19-mRNA-infographic_G_508.pdf
[*8] https://stratagemsoftheright.blogspot.com/2021/04/to-get-or-not-get-not-vaccine-anatomy.html
[*9] https://openontario.ca/articles/2021/06/23/dr-mercola-explains-dr-bridles-bombshell-revelations-regarding-spike-proteins
[*10] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (p. 132). Chelsea Green Publishing. Kindle Edition.
[*11] https://www.statnews.com/2017/01/10/moderna-trouble-mrna/
[*12] https://www.biologicalmedicineinstitute.com/post/covid-19-mrna-vaccines
[*13] https://www.fda.gov/media/144245/download
[*14] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (pp. 134-135). Chelsea Green Publishing. Kindle Edition.
[*15] https://abc7news.com/cape-cod-covid-outbreak-cdc-mask-guidance-face-masks-delta-variant/10918914/
[*16] https://stratagemsoftheright.blogspot.com/2021/05/what-to-consider-before-getting-covid.html
[*17] https://www.amazon.com/Truth-About-COVID-19-Lockdowns-Passports-ebook/dp/B08WRDXLVY Mercola, Joseph; Cummins, Ronnie. The Truth About COVID-19 (p. 138). Chelsea Green Publishing. Kindle Edition.
[*18] https://stratagemsoftheright.blogspot.com/2021/05/covid-19-not-vaccines-represent-41-of.html
[*19] https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
[*20] https://wonder.cdc.gov/vaers.html
[*21] https://stratagemsoftheright.blogspot.com/2021/05/covid-19-not-vaccines-represent-41-of.html
[*22] https://www.usatoday.com/story/news/factcheck/2020/04/24/fact-check-medicare-hospitals-paid-more-covid-19-patients-coronavirus/3000638001/









Comments
Post a Comment